

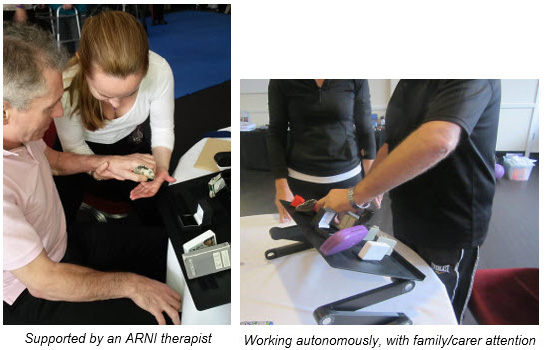
All therapists know what a challenge it is to try and help patients gain further action control of the more-affected upper limb. For ultra-effective upper limb training, get your task-specific training board shown here in conjunction with stretching before and after each grasp and release sequence.
 If you or your loved one has upper limb limitations, this can be an excellent way to ‘increase the dosage’ of repetitions.
If you or your loved one has upper limb limitations, this can be an excellent way to ‘increase the dosage’ of repetitions.
As Professor Nick Ward at the Institute of Neurology points out continually, in his and his team’s efforts to get stroke survivors to do more to engage the upper limb, ramping up the amount of grasp and release efforts performed daily may be most likely to increase neuroplasticity and accelerate recovery.
At last, available to you is the Upper Limb Task-Training board, as described in Successful Stroke Survivor and accompanying DVDs.
An innovative and simple idea created by Dr Tom Balchin which has helped thousands of survivors around the world since 2011, is now standardised here for you with his ideas of optimal content.
 Red, Pink or Silver: choose your colour for a Christmas gift to yourself or another!
Red, Pink or Silver: choose your colour for a Christmas gift to yourself or another!
Comes with a full colour, fully illustrated 10-page A4 GUIDE for use.
The laptop tray, which can be opened and locked at any angle, is covered with strategically placed Velcro hook and comb strips and squares. 11 different tactile items, each with different manual challenge, have been sourced and purchased for stroke survivors to practice grasp, place and release.
 These are really great for people to try, if there is spasticity or flaccidity present – and this is the stepping stone that we have found for countless ARNI patients over the years that works to progress their hand from one phase to another. Best advice is always start off with the wooden pegs in slots. Physiotherapists have, among their many upper limb measures, a test called the ‘9 hole peg test’. This is an idea borrowed and scaled up from that test, with slots to enable practice. Advice is (all present in the Guide), is to start off with these, working on ‘getting the gap’.
These are really great for people to try, if there is spasticity or flaccidity present – and this is the stepping stone that we have found for countless ARNI patients over the years that works to progress their hand from one phase to another. Best advice is always start off with the wooden pegs in slots. Physiotherapists have, among their many upper limb measures, a test called the ‘9 hole peg test’. This is an idea borrowed and scaled up from that test, with slots to enable practice. Advice is (all present in the Guide), is to start off with these, working on ‘getting the gap’.
 Dr Tom shows you in the Guide how to try create the temporary ability via a particular stretching sequence how to maintain a gap between thumb, index and middle finger to enable a grasp upon command. The idea is to work up to being able to go up and down the line, lifting and replacing.
Dr Tom shows you in the Guide how to try create the temporary ability via a particular stretching sequence how to maintain a gap between thumb, index and middle finger to enable a grasp upon command. The idea is to work up to being able to go up and down the line, lifting and replacing.
When you can do this, it’s time to move on to more challenging items on the board. The longest, smoothest and widest items are the most challenging. The Velcro always keep the paretic hand from knocking over items as the survivor attempts to grasp items until more fluidity/accuracy is gained. All is explained in the Guide and DVDs. You are going to like this approach; it gives SERIOUS RESULTS in terms of action control.
This is a must-have for all stroke survivors with upper limb limitations.
Sourcing the varying of thickness and adhesiveness of very high-strength Velcro, the cost of the lockable laptop board itself, combined with the cost of the items adds up surprisingly. We have done all this and put the time in to create and offer you this at the very best possible price to cover outlay.
Get yours here to help yourself or your loved one with ARNI style upper-limb training… and get a fully-illustrated colour 10 page accompanying Guide with it!
Go to the Products page to get the Task-Board.
IMPORTANT – Instructors and survivors will also be using this board together for forthcoming upper-limb telerehab sessions.

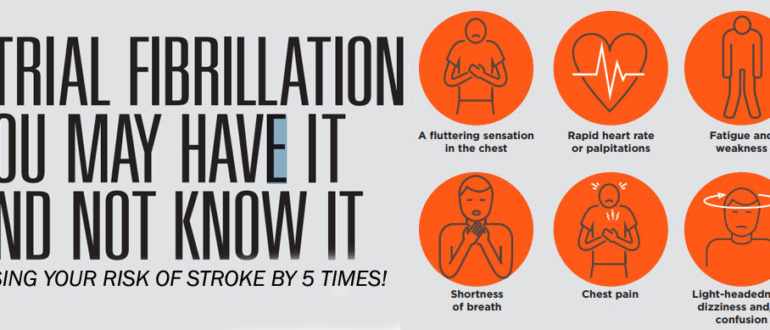
 Given that around 1 in 5 women, and around 1 in 6 men will have a stroke in their life, you really need to be aware and checking up on this.
Given that around 1 in 5 women, and around 1 in 6 men will have a stroke in their life, you really need to be aware and checking up on this.


 The 13th UK Stroke Forum Conference takes place at The International Centre, Telford, from 4 – 6 December 2018 and it welcomes stroke survivors who want to find out more about how to tackle their residual limitations.
The 13th UK Stroke Forum Conference takes place at The International Centre, Telford, from 4 – 6 December 2018 and it welcomes stroke survivors who want to find out more about how to tackle their residual limitations.
 Come and see us at the ARNI table at the Charities section! We have been running a table for 10 years at this outstanding Conference.
Come and see us at the ARNI table at the Charities section! We have been running a table for 10 years at this outstanding Conference. 
 If you need to know a little more about Conference before registering interest/calling the Stroke Association, please email tom@arni.uk.com and I’ll do my best to help with questions/steer to the right person at Stroke Association who can answer your question(s) asap…
If you need to know a little more about Conference before registering interest/calling the Stroke Association, please email tom@arni.uk.com and I’ll do my best to help with questions/steer to the right person at Stroke Association who can answer your question(s) asap…

 Like so many people, I didn’t really know much about strokes. I didn’t understand what they were and what effects they have. I thought it was something that only affects the old and unhealthy. I was very very wrong. Strokes can happen to anybody, any age, any fitness, any race. It does not distinguish between how much money you have, how good of a person you are or what your religion is. When it strikes, it strikes without warning, without prejudice and without mercy.
Like so many people, I didn’t really know much about strokes. I didn’t understand what they were and what effects they have. I thought it was something that only affects the old and unhealthy. I was very very wrong. Strokes can happen to anybody, any age, any fitness, any race. It does not distinguish between how much money you have, how good of a person you are or what your religion is. When it strikes, it strikes without warning, without prejudice and without mercy.


 Early discharges from hospitals are a good idea to free up hospital beds and to get you back to familiar surroundings once again. But only if the support mechanism of your further ‘re-training’ is in place. Often the support can finish too quickly, leaving survivors (and usually their families/carers too) worried about what to do next, and who to go to for further help. Outpatient therapy and community care, or the lack of it, is often quite wrongly, blamed for not solving all problems.
Early discharges from hospitals are a good idea to free up hospital beds and to get you back to familiar surroundings once again. But only if the support mechanism of your further ‘re-training’ is in place. Often the support can finish too quickly, leaving survivors (and usually their families/carers too) worried about what to do next, and who to go to for further help. Outpatient therapy and community care, or the lack of it, is often quite wrongly, blamed for not solving all problems. This information will include a summary of your rehabilitation progress and your current goals, your diagnosis and your current health status. Functional abilities, which include communication needs are included as well as your care needs – washing, dressing, going to the toilet, eating and so on.
This information will include a summary of your rehabilitation progress and your current goals, your diagnosis and your current health status. Functional abilities, which include communication needs are included as well as your care needs – washing, dressing, going to the toilet, eating and so on.
 Aphasia is more common than you might think.
Aphasia is more common than you might think. The PLORAS research study
The PLORAS research study Updates on the progress of their research can be found on their
Updates on the progress of their research can be found on their 
 Welcome to the new Data Laws coming in to effect tomorrow: May 25th.
Welcome to the new Data Laws coming in to effect tomorrow: May 25th.

 For a participant, the study will begin with a researcher attending the participants in their homes to perform a baseline assessment. One week later the researcher will deliver the Gameball device and train the participant how to use the device. The participant will then be asked to progressively increase the amount of time they use the device over the first week they have it. After that first week the participants will be asked to use the device as much as safely possible for 6 weeks. The participant will have the Gameball for a total of 7 weeks before the researcher then collects the Gameball and performs an assessment. The researcher will return 4 weeks later to perform a final follow up assessment. The total process will last 12 weeks.
For a participant, the study will begin with a researcher attending the participants in their homes to perform a baseline assessment. One week later the researcher will deliver the Gameball device and train the participant how to use the device. The participant will then be asked to progressively increase the amount of time they use the device over the first week they have it. After that first week the participants will be asked to use the device as much as safely possible for 6 weeks. The participant will have the Gameball for a total of 7 weeks before the researcher then collects the Gameball and performs an assessment. The researcher will return 4 weeks later to perform a final follow up assessment. The total process will last 12 weeks.



 The aim for this study is to research a treatment method to see if can improve upper limb function.
The aim for this study is to research a treatment method to see if can improve upper limb function.